





Lateral Mass Screws Fixation of Cervical Spine
Lateral mass screw fixation of cervical spine was first introduced by Roy-Camille et al. in the 1980s.
* Surgical Indications
1) Trauma: – Unstable fractures
2) Reconstruction: Tumors / Osteomyelitis / Inflammation (Rheumatoid Arthritis )
3) Degenerative Conditions: Combined posterior decompression / adjacent multilevel fixation
4) Pediatric Spine: Congenital Malformation
Surgery Video:

* Important Questions should be considered when choosing the operative approach
Question (1) : What is the alignment of the c ervical spine? Lordotic, Straight or Kyphotic?
– Posterior decompression without fixation is primarily indicated for lordotic and possibly straight spinal configurations.
Question (2) : How rigid is the deformity?
– A single-stage posterior approach with stabilization remains an option even in the presence of kyphosis if postural reduction restores sagittal balance.
– Fixed kyphotic deformities are an absolute contraindication to the posterior approach.
Question (3) : What is the nature of the pathologic process? How many spinal levels are involved? Does the patient have congenital stenosis?
– Anterior interbody strut grafting beyond two levels is associated with an increased failure rate, in such cases supplemental posterior stabilization is required, or a single-stage posterior approach my be more appropriate.
Question (4) : Does a static or mobile subluxation exist?
– Severe subluxation or any increase seen on dynamic imaging would eliminate the possibility of a standalone laminectomy and require inclusion of a stabilization and fusion.
Question (5) : What is the patient’s baseline medical status?
– Older patients typically more prone to swallowing dysfunction with anterior approaches, severe osteoporosis will increase the chance of grafting subsidence.
– In order patients, a posterior approach may be more appropriate.

Question (6) : Does the patient complain of significant axial neck pain?
– The presence of axial neck pain, if attributed to motion across a spondylotic segment, may support the addition of an arthrodesis.
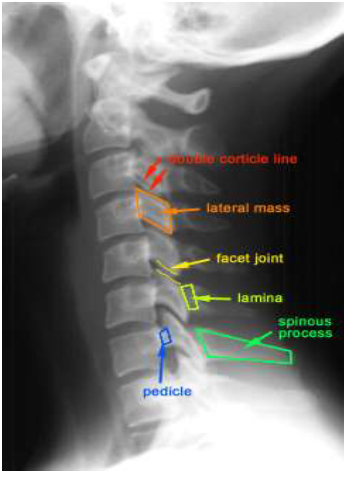
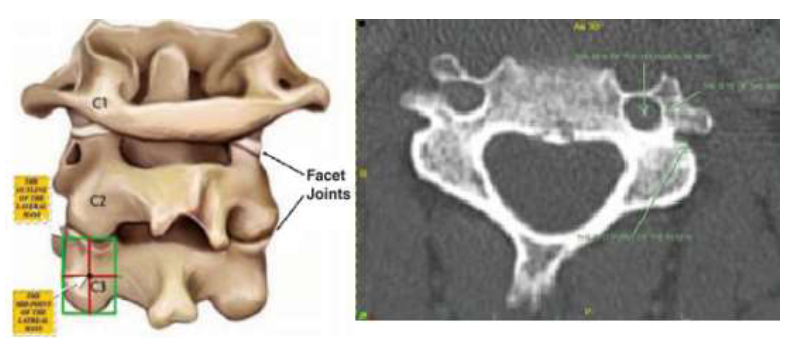
Lateral Mass Bony Structures: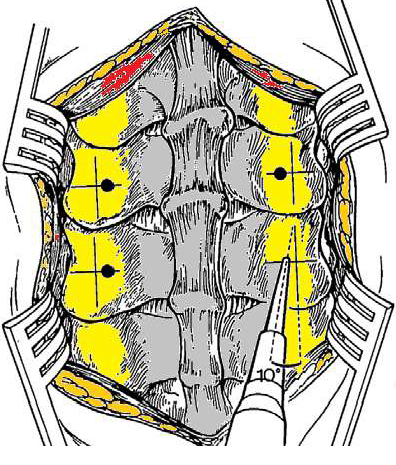
Consists of superior and inferior facets.
It is the part: – Lateral to the lamina.
– Between the inferior margins of the adjacent inferior facets.
Mean diameters of lateral mass:
 – Superoinferior from 11mm at C3 to 15mm C7.
– Superoinferior from 11mm at C3 to 15mm C7.
– Mediolateral from 12mm to 13mm at C3 through C7.
– Anterioposterior the lateral mass is smaller at the C6-C7 levels than at the levels above.
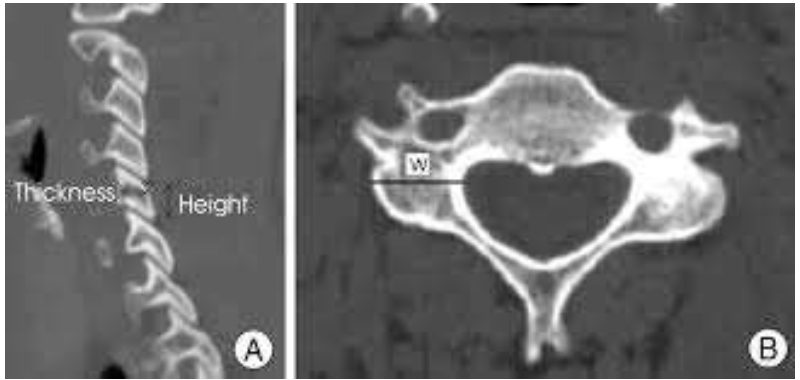 – Width: 12mm to 13mm at C3 through C7.
– Width: 12mm to 13mm at C3 through C7.
– Height: 11mm at C3 – 15mm C7
– Thickness: smaller at C6-C7 than levels above.
Lateral Mass Width:
– Range: 8.0 mm – 16.1 mm
– Mean width greater in males at all levels and greatest at C6 for males (12.8mm) and females (11.1mm)
Anterior to the lateral mass:
 – The Pedicle ( Anteromedially ),
– The Pedicle ( Anteromedially ),
– Transverse foramen,
– Posterior ridge of the transverse process ( Inferolaterally ) just above the inferior articular facet.
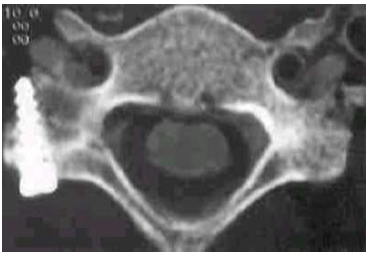
Transverse Foramen:
– Contains the vertebral artery, surrounded by:
* anterior ridge of transverse process anteriorly,
* the vertebral body medially,
* the pedicle, anterior wall of the lateral mass, and the posterior ridge of the transverse process posteriorly.
– C3-C5 : anteromedial to the posterior center of the lateral mass.
– at C6 : courses laterally and lies in front of the posterior center of the lateral mass.
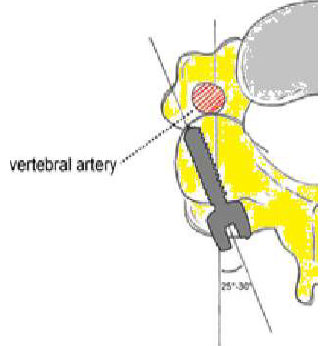
The vertebral artery:
– From the subclavian artery –> transverse foramen of C6 –> upward through the foramina above –> Deep in front of the lateral mass, separated by spinal nerve.
– Not at risk of injury as long as the screw is directed lateral in sagittal plane.
The interpedicular foramen:
– Formed by: * Adjacent pedicles,
* Posterolateral wall of vertebral body,
* Anteromedial aspect of the superior articular process.
The spinal nerve: Cervical Nerve Root
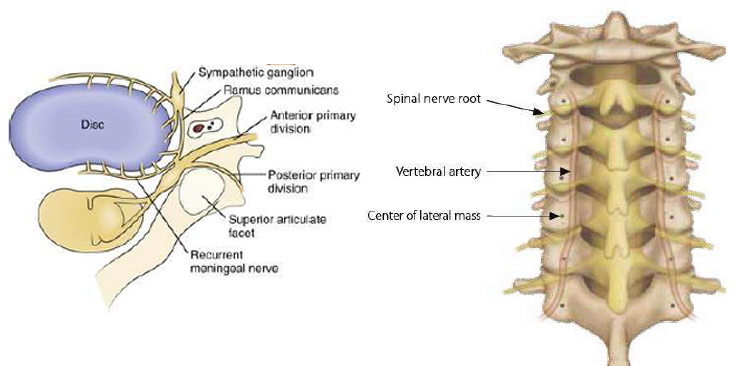
– Passes through the lower part of interpedicular foramen –> Laterally in the transverse foramen, it divides into a Larger anterior ramus and a smaller dorsal ramus.
– The ventral ramus courses on the transverse to form the cervical and brachial plexus.
The dorsal ramus:
– in the transverse foramen runs posteriorly against the corner of the base of the superior articular process
– Supplies –> the facet joint, ligaments, deep muscles, and the skin of the posterior aspect of neck.
– Diameter: * C3-C5: Larger (1.6mm – 2.2mm) * C6-C7: smaller (1.2mm)
Lateral Mass Quadrants:
The superolateral quadrant is away from spinal nerve and vertebral artery.
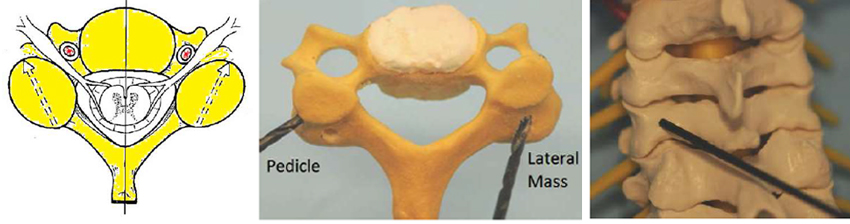
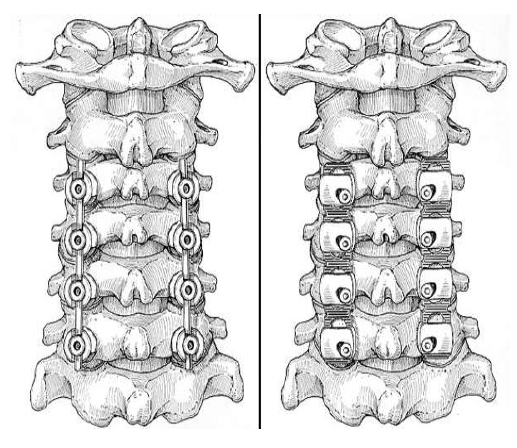
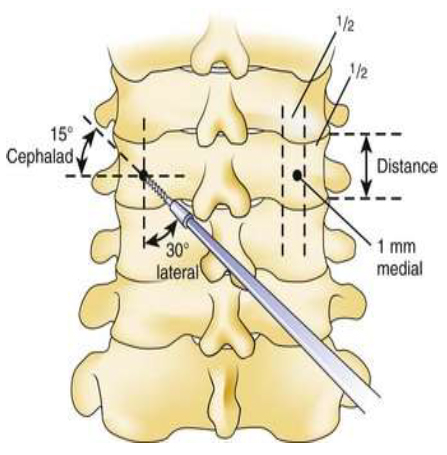
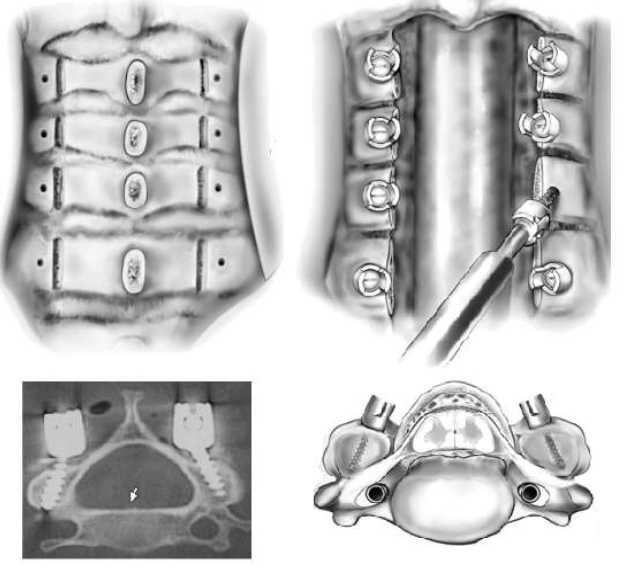
Lateral Mass Screws: (C3-C7)
– Starting point –> near center of lateral mass –> Direct screw tip up and lateral ( Away from the nerve root, spinal cord, and vertebral artery )
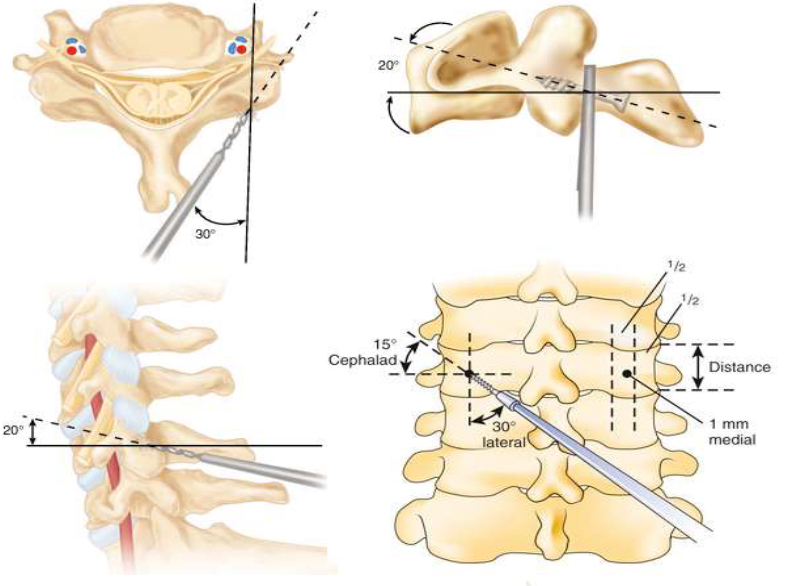
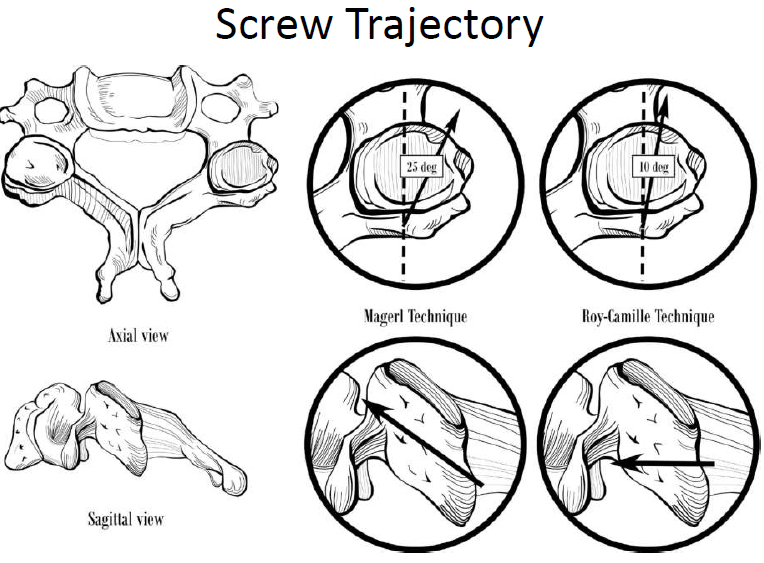
Magrel Screw
– Length: 6.3 – 20.4 mm
– Greater in males at all subaxial levels, greatest at C6 for males (15.6mm) and females (14.0mm), shortest at C7 for males (11.4mm) and females (9.6mm)
– Directed as lateral as superior as possible, to avoid injury to the spinal nerve and its dorsal ramus.
Roy-Camille Screw
– Length: 6.3 – 16.7 mm
– Greater in males at all subaxial levels, greatest at C5 for males (12.9mm) and C4 for females (11.5mm), shortest at C7 for males (9.8mm) and females (8.5mm)
– The exit point seems safe because it lies inferior to the dorsal ramus, and it’s separated from the ventral ramus by the posterior ridge of the transverse process.
Roy-Camille VS Magrel Screw
 – Magrel trajectory significantly longer than Roy-Camille trajectory.
– Magrel trajectory significantly longer than Roy-Camille trajectory.
– Average Magrel screw lengths: 2.6 mm longer at C3 – C6 levels, and 1.3 mm longer at C7 level.
Free hand technique of cervical lateral mass screw fixation:
Prof.Dr/Mohamed Mohi Eldin – Prof.Dr/Ahmed Salah Aldin Hassan
Read the full article here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5490344/
Lateral Mass screw efficiency
– High fusion success ( > 97%)
– Good maintenance of stability ( > 95%)
– Low complication rate: 10% increased kyphosis, rare hardware failure (except screws back out in plates )
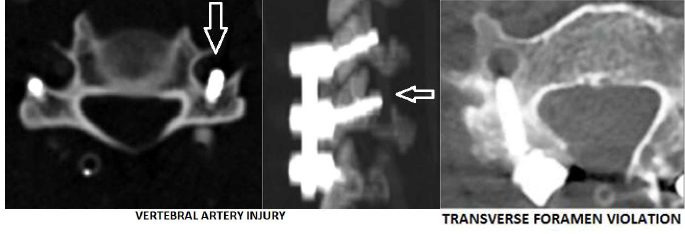
Lateral Mass screw safety
– Nerve root injury ( 1.2%), Vertebral artery injury (small risk)
Recommendations
– Template lateral mass screw length on image scans for determination of safe scew lengths at each level.

Anatomic Studies pediatric cervical screws:
– Feasibility based on anatomic dimensions does not prove safety.
– Vertebral canal dimensions > 80% of the adult level by 5 years of age.
– Growth arrest 2^ to screw placement across neurocentral synchondrosis leading to canal stenosis is not a concern.
Complications:
– Bleeding / Vascular injury.
– Neurologic injury.
– CSF Leak.
– Malposition.
– Implant loosening.
– Device breakage.
– Disassembly.
– Malfunction device.
– Bone Fractures.
– Graft settling / displacement.
– Loss of correction.
– Pseudoarthrosis.
– Wound infection.
– Skin irritation.
– Cardiac, Respiratory complications.
– Revision of surgery.
أضف تعليقك